Author: Dylan Krause, DO, Emergency Medicine Resident, PGY-1
Faculty: Alexis Cates, DO, Medical Toxicology/Emergency Medicine Attending
The Case:
A 35-year-old female with no significant past medical history presents to the emergency department complaining of shortness of breath and weakness that started several hours ago. The weakness is associated with chest tightness, congestion, hoarseness, and difficulty swallowing.
Of note, the patient also came to the emergency department 24 hours ago complaining of diplopia for one day. On that visit, she was discharged and was told to follow up with neurology. However, she continued to have persistent diplopia as well as new onset shortness of breath so returned for further evaluation.
Vitals: HR 75 bpm, BP 120/70, RR 10 bpm, SpO2 100% on room air, T 98.6F
Her physical exam is remarkable for bilateral ptosis of the eyelids and 4 out of 5 strength in bilateral upper extremities. Her strength in the lower extremities is 5 out of 5 bilaterally and her sensation is intact throughout. Her lungs are clear to auscultation bilaterally and cardiac exam is unremarkable. Laboratory work is ordered including complete blood count, complete metabolic panel, and urinalysis, all of which are within normal limits. Chest x-ray and computed tomography of her head do not show any acute abnormalities.
While you continue your workup for this patient, another patient presents to the emergency department similarly complaining of diplopia and muscle weakness. You begin to wonder if they are somehow connected and if so, what is causing these symptoms?
Learning Point 1: Will I ever encounter botulism in my emergency department?

Figure 1: Annual summary by the CDC of the number of botulism cases by state in 20182

Figure 2: Botulism cases recorded by the CDC in 2018 separated by transmission 2
In the United States, there are roughly 200 cases of botulism reported annually, according to the Centers for Disease Control and Prevention (CDC). Of these 200 cases, about 75% are infantile botulism and the other 25% are adult. Of the adult botulism cases approximately 20 are food borne and the remainder are associated with wounds. Of the infant botulism cases the main source is transmission by aerosolized botulinum spores in the soil. This typically happens near construction sites where the soil has been disturbed.
Botulism is caused by a toxin produced by Clostridium botulinum bacteria. These bacteria can produce the toxin in food, wounds, and the intestines of infants. The bacteria are also capable of making spores. These spores help the bacteria survive in the environment, even under extreme conditions. The spores usually do not cause adults to become sick. However if eaten or inhaled by children the spores can produce the toxin once ingested and cause symptoms, as their gastrointestinal tracts are not mature enough to handle contact with spores. .
Learning Point 2: What are the clinical manifestations of botulism?
Botulism has a variety of clinical manifestations. Some of the most common symptoms associated with adult botulism include:
- Diplopia
- Nausea
- Vomiting
- Sluggish pupils
- Dry mouth
- Ptosis
- Inability to produce facial expression
- Dysphagia
- Dysarthria
- Descending symmetric paralysis
In addition, there can be autonomic nervous system involvement in the form of constipation, urinary retention, and hypotension. Generally, patients retain normal mental status and sensory perception.
The signs of infant botulism vary from adult botulism. Possible signs of infant botulism can also include:
- Constipation
- Poor feeding
- Drooling
- Dysphagia
- Weak cry
- Lethargic
- Hypotonia (“floppy baby syndrome”)
Learning Point 3: What is the pathogenesis of botulism?
Botulinum toxin is produced by clostridium botulinum. This is a gram-positive, rod-shaped, spore-forming, anaerobic bacteria. These bacteria produce eight various types of toxin (A-H). The toxins are produced by spores which germinate under conditions with low oxygen exposure, pH of 7.0 or greater, and temperature between 25 -37 C. The spores are highly resistant to environmental stress once formed.
If the spores are ingested or inhaled by healthy adults, they are generally harmless. The same is not true for infants who have less developed gut microbiota. When infants ingest or inhale the spores, the toxins are then developed and released in vivo.
Once released or ingested, the mechanism of action of the toxins involves toxin-mediated blockade of neuromuscular transmission in cholinergic nerve fibers. The neurons take in the toxin via endocytosis as the heavy chain binds to receptors on the axon terminals. Then, the light chain of the botulism toxin clips SNARE proteins and inhibits the release of acetylcholine at the presynaptic clefts, as pictured in the figure below (Figure 3).
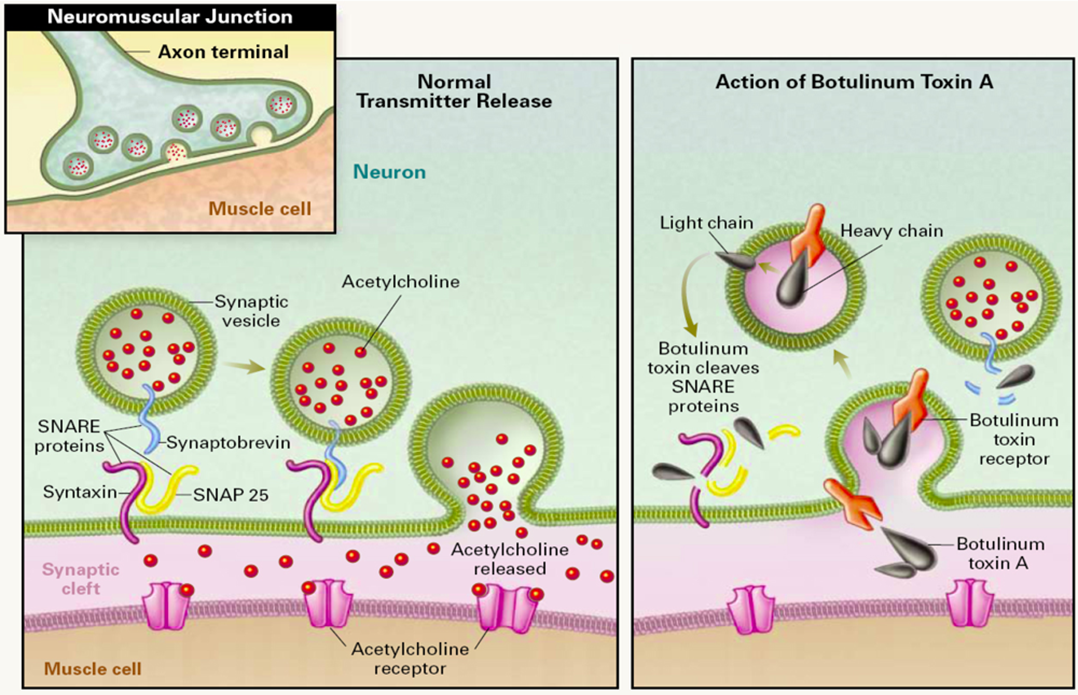
Figure 3: Mechanism of action of Botulinum toxin. The light chain of the toxin cleaves SNARE proteins and as a result prevents the release of ACh into the neuromuscular junction.5
The result of inhibiting acetylcholine release is a relaxed or flaccid muscle. The hypotonia continues to manifest as descending symmetric flaccid paralysis and is usually associated with gastrointestinal symptoms of nausea, vomiting, and diarrhea. The rate of mortality from botulism is low and if it does occur it is the result of paralysis to the diaphragm.
There are five major forms of botulism including: foodborne, wound, infantile, adult intestinal colonization, and iatrogenic. Botulism is extremely potent, only requiring 0.05 mcg of toxin to deliver potentially fatal symptoms.
Learning Point 4: How do I treat botulism?
The mainstay of treatment for botulism includes:
- Supportive care:
- Monitor vital signs closely
- Intubate when necessary
- Antitoxin administration:
- Adults and children greater than 1 year old:
- Heptavalent antitoxin
- Children less than 1 year old:
- BabyBIG (botulism immune globulin intravenous botulism antitoxin)
- Adults and children greater than 1 year old:
It is important to note that if the clinical suspicion for botulism infection is high you do not need to wait for lab results prior to administration of antitoxin. The antitoxin can be acquired from the local public health offices. These offices should also be contacted in the event of a potential outbreak.
The case concluded…
Now that you have a high clinical suspicion for botulism, you send out the botulinum toxin lab and symptomatic treatment is initiated. Her weakness progressively increased, and you decided to admit the patient to the hospital. While the patient is awaiting an inpatient bed her respiratory effort continues to worsen. She requires intubation, is placed on mechanical ventilation, and admitted to the intensive care unit.
Three days later, the botulinum toxin test came positive, and the patient was started on botulinum antitoxin. The Center for Disease Control (CDC) was contacted and tracked the events related to both patients admitted to your hospital. They discovered that they both had eaten nacho cheese from a gas station the day before the appearance of their symptoms.
There were eight other cases of botulism linked to nacho cheese from this same gas station in California in 2017. One died and the other nine were hospitalized. The mechanism of contamination for the nacho cheese still remains unclear. Common sources of foodborne botulism toxin are homemade foods that have been improperly canned, preserved, or fermented. Though uncommon, store-bought foods also can be contaminated with botulinum toxin.
Foods with low acid content are the most common sources of home-canning related botulism cases. These include asparagus, green beans, beets, corn, and potatoes. Botulism can be prevented in homemade foods by following safe home canning guidelines and using pressure canners for low-acid foods.
For infants, the most common infection from a food source is associated with honey. Again, it is not known how honey becomes contaminated with Clostridium Botulinum. It has been hypothesized that the spores, which are commonly found in soil and the environment, may be picked up by bees and they contaminate the honey.
Disclaimer: This case is based on a botulism outbreak that occurred in 2017 at a California gas station from nacho cheese.
References:
- Ho RY. BOTULISM. In: Olson KR, Anderson IB, Benowitz NL, Blanc PD, Clark RF, Kearney TE, Kim-Katz SY, Wu AB. eds. Poisoning & Drug Overdose, 7e. McGraw Hill; 2018. Accessed February 03, 2022. https://accessmedicine.mhmedical.com/content.aspx?bookid=2284§ionid=248385793
- Centers for Disease Control and Prevention (CDC). National Botulism Surveillance System Overview. Atlanta, Georgia: US Department of Health and Human Services, CDC, 2012.
- Jeffery IA, Karim S. Botulism. [Updated 2021 Jul 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459273/
- Choudhry SA, Anwar MJ, Afzal M, Shah A. Foodborne Botulism, I Only Had Nacho Cheese: A Case Report. Cureus. 2017;9(9):e1666. Published 2017 Sep 8. doi:10.7759/cureus.1666
Ali S. Al-Ghamdi, Noah Alghanemy, Hanan Joharji, Dhafer Al-Qahtani, Hasan Alghamdi. Botulinum toxin: Non cosmetic and off-label dermatological uses. Journal of Dermatology & Dermatologic Surgery. Volume 19, Issue 1. 2015. Pages 1-8. https://www.sciencedirect.com/science/article/pii/S2352241014000140#f0005
